|
After ACL reconstruction, the question everyone wants answered is simple:
When can I skate?
But that is not the best first question.
A better question is:
What does the knee need to show before skating makes sense?
Return to ice is not just about the calendar. It is about whether the knee is ready for the next dose.
A hockey player may be cleared by time, but not ready by criteria.
|
Return to ice should be earned. Not guessed.
|
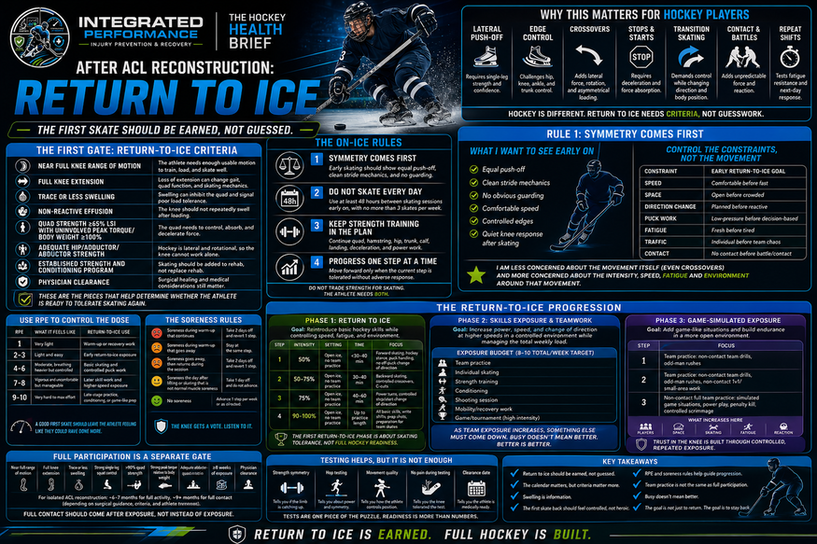
Why This Matters for Hockey Players
The research on ACL reconstruction specifically in hockey players is more limited than in sports like soccer, football, basketball, and handball.
That matters because hockey is different.
Skating has less vertical impact than running, but it still places a heavy demand on the knee. The ice can also hide problems early. A player may look fine during easy skating because glide helps them move. But when speed, direction change, fatigue, and contact are added, the knee has to work much harder.
| Hockey Demand |
Why It Matters After ACL Reconstruction |
| Lateral push-off |
Requires single-leg strength and confidence loading the involved side |
| Edge control |
Challenges hip, knee, ankle, and trunk control |
| Crossovers |
Adds lateral force, rotation, and asymmetrical loading |
| Stops and starts |
Requires deceleration and force absorption |
| Transition skating |
Demands control while changing direction and body position |
| Contact and board battles |
Adds unpredictable force and reaction |
| Repeat shifts |
Tests fatigue resistance and next-day response |
That is why return to ice needs criteria.
Not guesswork and hope.
Hope is not a strategy.
What the Research Tells Us
Return-to-sport rates after ACL reconstruction in elite and professional athletes are generally encouraging.
D’Ambrosi and colleagues reported that 85.8% of elite and professional athletes returned to play, with nearly 90% returning to their preinjury level. The pooled mean return time was 292 days, and the graft failure rate was 7.0%. [2]
Older hockey-specific professional data is also encouraging. Mai and colleagues reported that NHL players had the highest return-to-play rate across professional sports at 95.8%. [6]
But return rates are only part of the story.
Bloch and colleagues studied ACL reconstruction in men’s professional team sports, including ice hockey, and reported a high revision arthroscopy rate. Arthrofibrosis and cyclops formation were leading reasons for revision arthroscopy. [1]
That reinforces an important point:
| Research Reminder |
Practical Meaning |
| Many athletes return to sport |
Return is realistic, but it still needs to be earned |
| Revision arthroscopy can occur |
Early rehab foundations matter, especially restoring motion, managing swelling, and progressing appropriately |
| Graft failure risk still exists |
Time alone should not drive return-to-play decisions |
| Testing is helpful but imperfect |
Strength, movement quality, confidence, and sport exposure all matter |
|
Hockey Health Takeaway:
The research says many athletes get back. The rehab process helps decide how prepared they are when they do.
|
|
Part 1
The First Gate: Return-to-Ice Criteria
|
The first skate should not happen just because the athlete is excited, the season is close, or the calendar says it is time.
The knee should first show that it can tolerate load.
| Return-to-Ice Criteria |
Why It Matters |
| Near full knee range of motion |
The athlete needs enough usable motion to train, load, and skate well |
| Full knee extension |
Loss of extension can change gait, quad function, and skating mechanics |
| Trace or less swelling |
Swelling can inhibit the quad and signal poor load tolerance |
| Non-reactive effusion |
The knee should not repeatedly swell after loading |
| Quad strength ≥65% LSI with uninvolved peak torque/body weight ≥100% |
The quad needs to control, absorb, and decelerate force |
| Adequate hip/adductor/abductor strength |
Hockey is lateral and rotational, so the knee cannot work alone |
| Established strength and conditioning program |
Skating should be added to rehab, not replace rehab |
| Physician clearance |
Surgical healing and medical considerations still matter |
It may sound basic.
It is.
But these are still some of the most commonly missed steps in the return-to-ice process.
These are the pieces that help determine whether the athlete is ready to tolerate skating again.
Why These Criteria Matter
| Criteria Area |
What to Watch |
Hockey Translation |
| Motion |
Full extension, near full flexion, no movement compensation |
The athlete can access skating positions without changing mechanics |
| Swelling |
Trace or less, non-reactive response after activity |
The knee is tolerating the current dose |
| Quad strength |
Strong enough to control single-leg loading and absorb force |
The athlete can push, stop, and decelerate without protecting the knee |
| Single-leg control |
No knee collapse, trunk dumping, hip shift, or side-to-side avoidance |
The athlete can manage stride demands and directional changes |
| Hip and trunk capacity |
Strong hips, adductors, abductors, hamstrings, calf, and trunk |
The whole system supports the knee during lateral hockey movement |
|
Hockey Health Takeaway:
Swelling after skating is not just soreness. It is feedback.
|
Once the athlete is ready to skate, the next question becomes:
How do we dose it?
| Rule |
What It Means |
Why It Matters |
| Symmetry comes first |
Early skating should show equal push-off, clean stride mechanics, and no guarding |
The first phase is about quality. It sets our movement standard |
| Do not skate every day |
Use at least 48 hours between skating sessions early on, with no more than 3 skates per week |
The knee may feel fine during the skate but react later |
| Keep strength training in the plan |
Continue quad, hamstring, hip, trunk, calf, landing, deceleration, and power work |
The ice is part of rehab. It is not the whole rehab program |
| Progress one step at a time |
Move forward only when the current step is tolerated without adverse response |
Symptoms, swelling, or poor skating quality should guide the next dose |
|
Hockey Health Takeaway:
Do not trade strength for skating. The athlete needs both.
|
Rule 1: Symmetry Comes First
Early return-to-ice work should be simple enough that the athlete can move well.
That does not mean the athlete has to skate in a straight line forever.
It means we need to control the environment well enough that we can actually evaluate the movement.
In the early stages, I am watching for:
| What I Want to See |
What It Tells Me |
| Equal push-off |
The athlete is not avoiding the involved side |
| Clean stride mechanics |
The knee, hip, and trunk are working together |
| No obvious guarding |
The athlete trusts the movement enough to load it |
| Comfortable speed |
The drill is challenging but not overwhelming |
| Controlled edges |
The athlete can manage position without rushing |
| Quiet knee response after skating |
The dose was appropriate |
This is where the idea of controlling constraints matters.
The movement itself is not always the problem.
The question is:
| Constraint |
Early Return-to-Ice Goal |
| Speed |
Comfortable before fast |
| Space |
Open before crowded |
| Direction change |
Planned before reactive |
| Puck work |
Low-pressure before decision-based |
| Fatigue |
Fresh before tired |
| Traffic |
Individual before team chaos |
| Contact |
No contact before battle/contact exposure |
This is the difference between removing hockey movements and dosing hockey movements.
For example, I am not always worried about a crossover by itself.
I am more concerned about the intensity, speed, fatigue, traffic, and pressure around that crossover.
A slow, controlled crossover in open ice is very different from a full-speed crossover under pressure in a game.
Same movement.
Different dose.
|
Hockey Health Takeaway:
In early return to ice, symmetry comes first. The goal is not to avoid hockey movement forever. The goal is to find the version of the movement the athlete can own with quality, confidence, and a quiet knee response.
|
|
Part 3
Use RPE to Control the Dose
|
Rate of perceived exertion, or RPE, gives players, parents, coaches, and clinicians a shared language.
| RPE |
What It Feels Like |
Return-to-Ice Use |
| 1 |
Very light |
Warm-up or recovery work |
| 2–3 |
Light and easy |
Early return-to-ice exposure |
| 4–6 |
Moderate, breathing heavier but controlled |
Basic skating and controlled puck work |
| 7–8 |
Vigorous and uncomfortable but manageable |
Later skill work and higher-speed exposure |
| 9–10 |
Very hard to max effort |
Late-stage practice, conditioning, or game-like prep |
A good first skate should leave the athlete feeling like they could have done more.
The goal is not to win the first session.
The goal is to build moving forward.
|
Part 4
The Soreness Rules
|
The knee’s response determines the next step.
| Response |
What to Do |
| Soreness during warm-up that continues |
Take 2 days off and revert 1 step |
| Soreness during warm-up that goes away |
Stay at the same step |
| Soreness goes away, then returns during the session |
Take 2 days off and revert 1 step |
| Soreness the day after lifting or skating that is not normal muscle soreness |
Take 1 day off and do not advance |
| No soreness |
Advance 1 step per week or as directed |
This helps prevent the common mistake of stacking more work on top of a knee that is already irritated.
|
Hockey Health Takeaway:
The knee gets a vote. Listen to it.
|
|
Part 5
The Return-to-Ice Progression
|
The return-to-ice progression should move from controlled skating to controlled hockey exposure before full team play.
Do not jump from easy laps straight into full practice.
Phase 1: Return to Ice
Goal: Gradually reintroduce basic hockey skills while controlling speed, fatigue, and environment.
This phase is about rhythm, confidence, and skating tolerance.
One thing I have changed over time is how I think about early skating restrictions.
I used to be more focused on limiting what the athlete was allowed to do.
No crossovers.
No abrupt change of direction.
There is a place for that.
But I have found that once an athlete is in a safe place in rehab, the better approach is often not to remove every hockey movement. It is to control the constraints around the movement.
That means controlling the speed, space, fatigue, volume, traffic, and intensity of the drill.
Take crossovers as an example.
Crossovers do carry a level of risk. They challenge the knee, hip, trunk, edge control, rotational control at the knee, and confidence. But if the athlete has met return-to-ice criteria, is skating in an open environment, is moving at a comfortable speed, and is not reacting to pressure, I am usually less concerned about the crossover itself.
I am more concerned about how intensely they are doing it.
A slow, controlled crossover in open ice is very different from a full-speed crossover under pressure in a game.
Same movement.
Different dose.
Early return to ice should not be about avoiding every hockey movement forever. It should be about finding a version of the movement the athlete can perform with quality, confidence, and a quiet knee response.
| Instead of Only Saying “No” |
Control the Constraint |
| No crossovers |
Crossovers at comfortable speed in open ice |
| No change of direction |
Planned direction changes before reactive ones |
| No stops and starts |
Controlled stop/start work before high-speed stops |
| No puck work |
Low-pressure puck handling before decision-based drills |
| No shooting |
Wrist and snap shots before harder slap shots or one-timers |
| No team drills |
Individual skills before traffic, pressure, and contact |
The goal is to reintroduce hockey movements in a way the athlete can own.
Not rushed.
Not chaotic.
Not max effort.
Controlled enough to build confidence.
Specific enough to actually prepare them for hockey.
A sample progression may look like this:
| Step |
Intensity |
Setting |
Time |
Focus |
| 1 |
50% |
Open ice, no team practice |
Under 30–40 min |
Forward skating, hockey turns, puck handling, no abrupt change of direction |
| 2 |
50–75% |
Open ice, no team practice |
30–40 min |
Backward skating, controlled crossovers, C-cuts |
| 3 |
75% |
Open ice, no team practice |
40–60 min |
Power turns, controlled stop/start change of direction |
| 4 |
90–100% |
Open ice, no team practice |
Up to practice length |
All basic skills, wrist shots, snap shots, preparation for team skates |
The first return-to-ice phase is about skating tolerance, not full hockey readiness.
I want the athlete to get off the ice and feel successful.
That confidence matters.
|
Hockey Health Takeaway:
The movement is not always the problem. The dose, speed, fatigue, and environment usually decide whether the movement is appropriate.
|
Phase 2: Skills Exposure and Teamwork
Goal: Increase power, speed, and change of direction at higher speeds in a controlled environment while managing the total weekly load.
This is where the athlete starts to rejoin the hockey environment.
It is also where families can get into trouble.
The athlete feels better.
The knee looks better.
Team practice is back on the calendar.
Individual skills are still happening.
Strength training is still needed.
Conditioning starts creeping back in.
Shooting sessions get added because the player “missed time.”
All of a sudden, the athlete is doing more than they were before the injury.
That is a load spike.
This connects directly back to Newsletter #3:
|
Busy does not mean better. Better is better.
|
During this phase, the goal is not to collect as many exposures as possible. The goal is to dose the right exposures so the athlete can adapt.
A good target is still roughly 8–10 total athletic exposures per week, but only 3–4 should feel truly high intensity.
For an ACL athlete in Phase 2, those exposures might include:
| Exposure Type |
Counts as an Exposure? |
Why It Matters |
| Team practice |
Yes |
Adds speed, timing, teammates, and hockey environment |
| Individual skating |
Yes |
Builds controlled skill quality and confidence |
| Strength training |
Yes |
Keeps rebuilding the knee, hip, trunk, and lower body |
| Conditioning |
Yes |
Adds fatigue and repeat-effort demand |
| Shooting session |
Yes |
Adds volume, rotation, single-leg loading, and fatigue |
| Mobility or recovery work |
Yes, if structured |
Helps manage tissue response and restore quality |
| Tournament/game exposure |
Yes, high intensity |
Should change the rest of the week |
The body counts all of it.
Not just the skates.
Phase 2 Exposure Budget
As team exposure increases, something else usually needs to come down.
That is the key.
| Phase 2 Step |
Team Exposure |
Individual Work |
Load Management Point |
| Step 1 |
Team practice 1x/week |
Individual drills 3x/week |
Most work is still controlled and individual |
| Step 2 |
Team practice 2x/week |
Individual drills 2x/week |
Team exposure increases, so individual volume decreases |
| Step 3 |
Team practice 3x/week |
Individual drills 1x/week |
The week is becoming more hockey-heavy |
| Step 4 |
Full-time team practice |
Individual work as needed |
Extra work should be selective, not automatic |
This is the part that matters:
|
Do not add team practice on top of everything else.
|
Replace some of the individual work with team exposure.
That is how the athlete progresses without turning the week into a fatigue problem.
What Should Stay In During Phase 2?
The athlete still needs a complete plan.
But the dose matters.
| Training Piece |
Keep It? |
How to Think About It |
| Team practice |
Yes |
Progress gradually from limited exposure toward full-time practice |
| Individual skating |
Yes |
Use it to clean up skills, confidence, and mechanics |
| Strength training |
Yes |
Do not abandon the strength plan when skating increases |
| Power and deceleration |
Yes |
Keep building the qualities needed for stops, starts, and transitions |
| Conditioning |
Maybe |
Add carefully, because practice already creates conditioning stress |
| Extra shooting |
Maybe |
Useful, but it still counts as load |
| Recovery day |
Yes |
Needed to absorb the work and monitor the knee response |
The mistake is not doing these things.
The mistake is doing all of them at full volume in the same week.
Skill Work vs. Conditioning
Another mistake in this phase is accidentally turning every skill session into a conditioning session.
That matters after ACL reconstruction.
If the goal is skill exposure, the athlete should be fresh enough to move well, make decisions, and build confidence.
If fatigue takes over, mechanics can change.
The athlete may start avoiding one side, shortening the stride, losing edge quality, or hesitating with stops and starts.
That is not quality return-to-ice work.
That is just getting tired.
| Session Type |
Main Goal |
What Quality Looks Like |
| Individual skill session |
Clean movement and controlled exposure |
Good mechanics, confidence, quiet knee response |
| Team practice |
Timing, spacing, and hockey environment |
Athlete participates without guarding or swelling response |
| Conditioning exposure |
Build repeat-effort tolerance |
Fatigue is expected, but mechanics should not fall apart |
| Recovery session |
Restore quality |
Athlete feels better after, not more irritated |
All of these can be useful.
They are not the same thing.
Phase 2 Weekly Example
Here is what a reasonable week could look like.
This is not a perfect plan for every athlete, but it shows the idea.
| Day |
Exposure |
Intensity |
Purpose |
| Monday |
Strength training |
Moderate |
Build quad, hip, trunk, and lower-body capacity |
| Tuesday |
Individual skating |
Moderate |
Skill quality, transitions, controlled power turns |
| Wednesday |
Recovery / mobility |
Low |
Let the knee respond and restore quality |
| Thursday |
Team practice |
Moderate to high |
Timing, flow, controlled team exposure |
| Friday |
Strength + deceleration work |
Moderate |
Keep building force absorption |
| Saturday |
Individual skating or shooting |
Low to moderate |
Controlled skill work, not conditioning |
| Sunday |
Off or recovery |
Low |
Absorb the week |
That is 6–7 structured exposures.
If the athlete is tolerating the week well, another low or moderate exposure may fit.
If team practice increases to 2–3 times per week, the individual skating or conditioning volume should usually come down.
|
The goal is not to max out the calendar.
|
The goal is to stack quality work and let the knee adapt.
Phase 2 Guardrails
| If This Happens |
Adjust This |
| Knee swells after practice |
Reduce team exposure or total weekly volume |
| Skating quality drops late in sessions |
Shorten the session or reduce intensity |
| Athlete avoids one side |
Return to controlled individual work |
| Strength numbers stall |
Protect strength training instead of adding more ice |
| Athlete looks tired all week |
Reduce high-intensity exposures |
| Symptoms are worse the next day |
Repeat the current step before progressing |
| Confidence improves and knee stays quiet |
Progress one variable at a time |
The biggest mistake in Phase 2 is progressing everything at once.
Do not increase team practice, individual skating, conditioning, shooting volume, and intensity in the same week.
Pick one variable.
Build it.
Watch the response.
Then decide what comes next.
|
Hockey Health Takeaway:
In Phase 2, the win is not doing more. The win is adding the right hockey exposure while keeping the knee quiet, strong, and confident.
|
Phase 3: Game-Simulated Exposure
Goal: Add game-like situations and build endurance in a more open environment.
This phase begins to look more like hockey.
| Step |
Setting |
Focus |
| 1 |
Team practice |
Non-contact team drills, odd-man rushes |
| 2 |
Team practice |
Non-contact team drills, odd-man rushes, non-contact 1v1 small-area work |
| 3 |
Non-contact full team practice |
Simulated game situations, power play, penalty kill, controlled scrimmage |
| What Increases Here |
Why It Matters |
| More players |
More visual processing and decision-making |
| More speed |
Greater force and faster reactions |
| More spacing |
More hockey-like movement problems |
| More fatigue |
Tests whether mechanics hold up |
| More reaction |
Builds trust in the knee |
This is where trust in the knee really matters.
|
Part 6
Full Participation Is a Separate Gate
|
Full participation is not automatic just because the athlete has returned to team practice.
For isolated ACL reconstruction, a practical timeline may be around 6–7 months for full activity and closer to 9+ months for full contact, depending on surgical guidance, criteria, and athlete response.
| Full Participation Criteria |
Why It Matters |
| Near full range of motion |
The athlete can access hockey positions |
| Full knee extension |
Helps normalize gait, skating mechanics, and quad function |
| Trace or less non-reactive effusion |
The knee is not reacting poorly to the current workload |
| Strong single-leg squat control to deeper range |
Shows better single-leg capacity and frontal-plane control |
| 90% or greater quad symmetry |
Raises the strength standard for full return |
| Strong peak torque relative to body weight |
Shows the athlete has usable strength, not just side-to-side symmetry |
| Adequate adductor-to-abductor strength ratio |
Supports lateral hockey movement |
| At least 8 weeks of exposure time |
Gives the athlete time to adapt to skating, practice, and team demands |
| Physician clearance |
Medical and surgical factors still guide progression |
That exposure time matters.
The athlete needs enough time to adapt to skating, practice, skill exposure, and team demands before full contact.
You cannot cram that into one week.
|
Hockey Health Takeaway:
Full contact should come after exposure, not instead of exposure.
|
|
Part 7
Testing Helps, But It Is Not Enough
|
Return-to-sport testing matters.
But testing is not perfect.
Solie and colleagues highlighted that current objective return-to-sport tests are useful, but they do not reliably predict safe return by themselves. [4]
Girdwood and colleagues also showed that people are more variable than hop tests alone would suggest after ACL reconstruction. [8]
| Test Result |
What It Tells You |
What It Does Not Fully Tell You |
| Strength symmetry |
Whether the involved limb is catching up |
Whether the athlete can use that strength in hockey |
| Hop testing |
Power, landing, and limb symmetry information |
Whether the athlete can handle contact, reaction, and fatigue |
| Movement quality |
How the athlete controls position |
Whether it holds up under game speed |
| No pain during testing |
The knee tolerated that test |
Whether the knee tolerates repeated hockey sessions |
| Clearance date |
The athlete is far enough along medically |
Whether the athlete is prepared for hockey chaos |
Two athletes may both pass a hop test.
One may skate confidently, stop hard, crossover both ways, absorb contact, and recover well.
The other may hesitate, avoid one side, swell after practice, or lose mechanics when tired.
Those are not the same athlete.
|
Hockey Health Takeaway:
Do not reduce return to hockey to one hop test, one strength number, or one date.
|
Not every symptom is a crisis.
But repeated signs matter.
| Warning Sign |
What It May Mean |
| Swelling after skating |
The knee may not be tolerating the current dose |
| Loss of knee extension |
The knee may be irritated or not recovering well |
| Pain that increases during activity |
The workload may be too high |
| Asymmetrical skating |
The athlete may be avoiding the involved side |
| Hesitation with stops and starts |
Confidence, strength, or deceleration may not be ready |
| Poor deceleration mechanics |
The athlete may not be absorbing force well |
| Knee collapse with landing or cutting |
Frontal-plane control may need more work |
| Heavy legs early |
Fatigue may be exposing a capacity issue |
| Symptoms worse the next day |
Recovery response is not ready for progression |
| Looks different when tired |
The athlete may not be ready for higher intensity or volume |
These signs do not mean the athlete failed.
They mean the progression gave you information.
Use it.
Adjust the dose.
Do not just keep adding.
Key Takeaways
| Key Point |
Why It Matters |
| Return to ice should be earned, not guessed |
The knee needs to meet criteria before skating progresses |
| The calendar matters, but criteria matter more |
Time alone does not equal readiness |
| Swelling is information |
A reactive knee is telling you the dose may be too high |
| Motion and quad strength set the foundation |
These drive mechanics, control, and confidence |
| The first skate back should feel controlled, not heroic |
Early return is about tolerance, not toughness |
| RPE helps dose the return |
It keeps intensity understandable and trackable |
| Soreness rules guide progression |
They reduce guessing after symptoms |
| Team practice is not the same as full participation |
Practice exposure still needs to be progressed |
| Full contact should come after exposure time |
The athlete needs repeated, successful exposures first |
| Cleared does not always mean prepared |
Medical clearance and sport readiness are not identical |
| Busy does not mean better |
The right exposures matter more than maxing out the calendar |
Final Thought
ACL reconstruction can help hockey players get back to the sport they love.
But return to hockey should not be rushed because the player feels good, misses the team, or hits a date on the calendar.
The knee has to earn the next step.
| The Process |
The Goal |
| Motion |
Move well |
| Swelling control |
Stay quiet |
| Strength |
Absorb and produce force |
| Single-leg control |
Own the involved side |
| Skating quality |
Move symmetrically |
| Exposure time |
Adapt to the sport |
| Confidence |
Trust the knee |
| Next-day response |
Prove the dose was appropriate |
| Total load management |
Stack quality work without creating a fatigue problem |
Skating is not the finish line.
Practice is not the finish line.
Even the first game back is not the finish line.
The goal is not just to return.
The goal is to stay back.
|
Return to ice is earned. Full hockey is built.
|
This Week’s Challenge
Pick the weakest link in the return-to-ice process.
| Possible Limiting Factor |
Next Step |
| Motion |
Restore the missing range before adding more load |
| Swelling |
Reduce the dose and monitor response |
| Quad strength |
Keep building force capacity |
| Skating symmetry |
Slow the progression and clean up mechanics |
| Stops and starts |
Rebuild deceleration before increasing speed |
| Confidence |
Add controlled exposure before chaos |
| Next-day response |
Repeat the current step instead of advancing |
| Weekly load |
Reduce total exposures or high-intensity exposures |
Find the limiting factor.
Then build the next step around it.
References
- Bloch H, Reinsberger C, Klein C, Luig P, Krutsch W. High revision arthroscopy rate after ACL reconstruction in men's professional team sports. Knee Surgery, Sports Traumatology, Arthroscopy. 2023;31(1):142-151. doi:10.1007/s00167-022-07105-0.
- D'Ambrosi R, Marchetti A, Farinelli L, et al. The majority of elite and professional athletes return to the preinjury level of activity after ACL reconstruction: a systematic review and meta-analysis. Knee Surgery, Sports Traumatology, Arthroscopy. 2025. doi:10.1002/ksa.70020.
- D'Ambrosi R, Marchetti A, Farinelli L, et al. Anterior cruciate ligament reconstruction in elite and professional athletes: does graft choice influence return to sport and failure rate? A systematic review and meta-analysis. International Journal of Surgery. 2026. doi:10.1097/JS9.0000000000004837.
- Solie BS, Tollefson LV, Doney CP, et al. Return to the pre-injury level of sport after anterior cruciate ligament reconstruction: a practical review with medical recommendations. International Journal of Sports Medicine. 2024;45(8):572-588. doi:10.1055/a-2270-3233.
- Sikka R, Kurtenbach C, Steubs JT, Boyd JL, Nelson BJ. Anterior cruciate ligament injuries in professional hockey players. American Journal of Sports Medicine. 2016;44(2):378-383. doi:10.1177/0363546515616802.
- Mai HT, Chun DS, Schneider AD, et al. Performance-based outcomes after anterior cruciate ligament reconstruction in professional athletes differ between sports. American Journal of Sports Medicine. 2017;45(10):2226-2232. doi:10.1177/0363546517704834.
- Ardern CL, Sonesson S, Forssblad M, Kvist J. Comparison of patient-reported outcomes among those who chose ACL reconstruction or non-surgical treatment. Scandinavian Journal of Medicine & Science in Sports. 2017;27(5):535-544. doi:10.1111/sms.12707.
- Girdwood MA, Crossley KM, Patterson BE, et al. People are more variable than their hop test would suggest: hop performance and self-reported outcomes over 11 years following ACL reconstruction. Scandinavian Journal of Medicine & Sports. 2024;34(9). doi:10.1111/sms.14727.
|